
Expertise
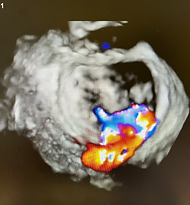
Echocardiography and Advanced Cardiac Ultrasound
Echocardiography (heart ultrasound) is one of the most important diagnostic tools in cardiology. It allows assessment of heart function, valve structure, and the movement of the heart walls.
It provides information about how well the heart pumps (ejection fraction), whether the heart muscle is functioning normally, and whether the valves are narrowed or leaking. Mild valve abnormalities are common and often not clinically relevant.
It is important to note that echocardiography cannot detect all heart diseases. For example, it does not reliably assess the coronary arteries, and normal findings do not completely exclude heart disease or rhythm disorders.
Stress echocardiography
Stress echocardiography evaluates heart function under increased workload. This is achieved by administering medication that stimulates the heart, simulating physical stress.
Under these conditions, reduced blood flow due to narrowed coronary arteries may become visible as abnormalities in heart wall motion. If the heart function remains normal under stress, significant coronary artery disease is less likely.
Transesophageal echocardiography (TEE)
Transesophageal echocardiography is performed via the esophagus, allowing higher image quality and more detailed visualization of heart structures.
This method is particularly useful for evaluating heart valves and detecting blood clots in the heart, for example in patients with atrial fibrillation. It is also often used before planned valve interventions when more precise imaging is required.



Cardiac CT (Coronary CT Angiography)
Cardiac CT is a non-invasive imaging method that allows detailed visualization of the coronary arteries using computed tomography. It enables detection of calcification and assessment of potential narrowing of the coronary vessels with high spatial resolution. The method is particularly useful in patients with a low to intermediate likelihood of coronary artery disease, where it can help reliably exclude significant vessel disease.
Cardiac CT is generally less suitable in patients with already known or advanced coronary artery disease, where other diagnostic methods may be more appropriate.
For optimal image quality, a low and stable heart rate is required, usually below 70 beats per minute during the examination.



Cardiac MRI
Cardiac MRI is an advanced imaging method that provides detailed information about the structure and function of the heart. Unlike CT, it does not use X-rays but works with magnetic fields and electromagnetic signals.
The examination typically takes 40–60 minutes and requires the patient to lie still, with repeated short breath-holds. In return, it offers excellent image quality and allows precise assessment of heart function, including measurement of the ejection fraction.
With the use of contrast agents, cardiac MRI can also detect and differentiate diseases of the heart muscle, such as inflammation, scarring, or cardiomyopathies.
Similar to stress echocardiography, stress testing can be performed using medication to evaluate blood flow to the heart muscle under increased workload.
Cardiac MRI is one of the most comprehensive tools in cardiology, although it has some limitations. It may be less suitable for patients with severe claustrophobia, inability to remain still, certain arrhythmias, or specific device-related restrictions. It also plays only a limited role in the direct diagnosis of cardiac rhythm disorders.



Coronary Angiography (Cardiac Catheterization)
What is coronary angiography?
Coronary angiography is an invasive diagnostic procedure that allows direct visualization of the coronary arteries.
A thin catheter is inserted through an artery in the arm or groin and advanced to the heart. Contrast medium is injected, and the vessels are displayed using X-ray imaging. This allows precise identification and assessment of narrowing.
When is it performed?
This procedure is typically used in patients with suspected or confirmed coronary artery disease, such as after a heart attack or when symptoms or prior tests indicate relevant vessel narrowing.
It may also be performed before certain cardiac procedures or to exclude coronary disease in specific clinical situations.
When is a stent needed?
If a significant narrowing is detected, treatment can often be performed immediately using balloon dilation and stent implantation.
However, not every narrowing requires treatment. If the severity is unclear, additional measurements (such as FFR or iFR/rFR) are used to determine whether the stenosis significantly limits blood flow.
What treatments are possible during the procedure?
Modern interventional cardiology allows treatment of a wide range of conditions, including:
-
stent implantation
-
treatment of heavily calcified vessels (e.g. rotablation)
-
chronic total occlusions (CTO interventions)
-
complex high-risk procedures with circulatory support (e.g. Impella)
Are there risks?
As with any invasive procedure, complications are possible but rare.
Serious complications such as vessel injury, heart attack, or stroke occur in less than 1% of cases. Minor complications, such as bleeding at the access site, may occur but are usually manageable.



Electrophysiological Study (EP Study)
What is an electrophysiological study?
An electrophysiological (EP) study is an invasive procedure used to diagnose and treat cardiac arrhythmias. It allows detailed analysis of the heart’s electrical system and is used when symptoms persist despite medication or when a curative treatment is preferred.
How does the procedure work?
Similar to cardiac catheterization, thin catheters are inserted through blood vessels and advanced to the heart under X-ray guidance. In contrast to coronary angiography, the access is usually via the venous system, allowing entry into the right side of the heart. Special electrodes are used to record electrical signals and analyze the origin and mechanism of the arrhythmia.
Can arrhythmias be treated during the procedure?
Yes. Once the source of the arrhythmia is identified, it can often be treated immediately. This is done using catheter ablation, where the responsible area is targeted with heat (radiofrequency) or cold (cryoablation) to interrupt the abnormal electrical pathway. Certain arrhythmias, such as atrial fibrillation or atrial flutter, have typical target areas that are treated using established techniques.
What are the limitations?
Not all arrhythmias can be treated with ablation, and success rates vary depending on the type of rhythm disorder. The decision to perform an EP study and ablation is always individualized based on symptoms, diagnosis, and expected benefit.
Are there risks?
As with any invasive cardiac procedure, there are potential risks, although serious complications are rare. These may include bleeding at the access site, vascular injury, or, in rare cases, complications similar to those seen in other catheter-based procedures.



Pacemakers, Defibrillators, and Cardiac Resynchronization Therapy
What are these devices?
These are implantable electronic devices used to support or regulate the heart’s rhythm and function.
-
Pacemakers stimulate the heart when the natural heart rate is too slow or pauses occur
-
Defibrillators (ICD) detect and treat life-threatening arrhythmias by delivering an electrical shock
-
Cardiac resynchronization therapy (CRT) improves coordination of heart contractions in patients with heart failure
When are they needed?
The indication for these devices is based on well-defined medical guidelines. They are used in specific situations, such as:
-
slow heart rate or conduction disturbances (pacemaker)
-
risk of dangerous arrhythmias or sudden cardiac death (ICD)
-
impaired heart function with dyssynchronous contraction (CRT)
The decision is always individualized but follows strict clinical criteria.
How are these devices implanted?
In most cases, electrodes (leads) are inserted through veins in the chest or arm and advanced into the heart under X-ray guidance. These leads are connected to a device placed under the skin in the chest area.
The system creates a direct electrical connection between the device and the heart, allowing continuous monitoring and, if necessary, intervention.
Are there newer device options?
Yes. Modern device therapy includes:
-
Leadless pacemakers, which are placed directly inside the heart without traditional leads
-
Subcutaneous defibrillators (S-ICD), where the electrode is placed under the skin without entering the heart
-
Conduction system pacing (e.g. left bundle branch area pacing, LBBAP), which allows more physiological activation of the heart
Not every device is suitable for every patient, and careful selection is essential.
What are the goals of therapy?
The aim is to:
-
maintain a stable heart rhythm
-
prevent dangerous arrhythmias
-
improve heart function and symptoms
-
reduce the risk of sudden cardiac death
Are there risks?
As with any invasive procedure, there are potential risks, including bleeding, infection, or lead-related complications. Serious complications are uncommon, and overall these procedures are considered safe and well established.

Transcatheter Valve Repair (TEER)
Transcatheter edge-to-edge repair (TEER) is a minimally invasive procedure used to treat certain types of valve regurgitation without open-heart surgery. During the procedure, a device is introduced through a vein in the groin and advanced to the heart under X-ray and transesophageal echocardiographic guidance.
The goal is to approximate (“clip”) specific parts of the valve leaflets to reduce the backward flow of blood. The exact position and feasibility of the repair are carefully assessed during the procedure.
TEER is technically demanding and not suitable for all types of valve disease. Careful patient selection is essential for a good outcome, and the procedure is typically considered when surgical treatment carries increased risk.
Although minimally invasive, the procedure is performed under anesthesia to ensure optimal precision. Hospital stay is usually short, with discharge often possible within one to two days.
The degree of improvement depends on individual anatomy and underlying disease. In many cases, regurgitation can be significantly reduced, although complete elimination cannot always be guaranteed.



Holter ECG and 24-Hour Blood Pressure Monitoring
Holter ECG and 24-hour blood pressure monitoring are widely used, non-invasive diagnostic methods that provide additional information beyond a single measurement.
A Holter ECG records the heart rhythm continuously over 24 hours or longer. This is particularly useful in patients with suspected arrhythmias, as it increases the likelihood of capturing intermittent rhythm disturbances during daily activities.
Similarly, 24-hour blood pressure monitoring provides a more accurate assessment of blood pressure control throughout the day and night. It helps determine whether current treatment is effective and may guide adjustments in therapy if elevated average values are detected.
These methods are commonly available and are often arranged through primary care physicians or cardiology practices.
